How to Tell If a Wound Is Infected (Evidence-Based Visual Guide)
16 min read · Updated May 2025
On this page
- 1. Real-Life Scenarios: When Normal Healing Takes a Turn
- 2. Quick Reference Guide
- 3. The Science of Infection vs. Healing
- Understanding Normal Wound Healing
- How Infection Disrupts Normal Healing
- 4. Visual Comparison: Normal Healing vs. Infection
- Normal Wound Healing Timeline with Visual Markers
- Warning Signs of Infection (Visual Indicators)
- 5. Evidence-Based Assessment Tool: Is Your Wound Infected?
- 6. Proper Wound Care Protocols to Prevent Infection
- Initial Wound Care
- Ongoing Care
- 7. High-Risk Wounds: When Standard Rules Don’t Apply
- High-Risk Wound Types
- High-Risk Patient Factors
- 8. Evidence-Based Home Care Products
- 9. When to Seek Professional Care: Decision Tree
- 10. Nutrition & Lifestyle Factors That Prevent Infection
- Evidence-Based Nutritional Support
- Lifestyle Factors That Significantly Impact Infection Risk
- 11. Comprehensive FAQ: Expert Answers
- 12. Expert Perspectives on Wound Infection
- 13. Resources & Top Articles:
- 14. Comprehensive Summary
- 15. References and Further Reading
Medical Disclaimer: This content is for informational purposes only and is not a substitute for professional medical advice. Always consult healthcare professionals for medical concerns.
1. Real-Life Scenarios: When Normal Healing Takes a Turn
Alex was preparing dinner when he sliced his finger with a kitchen knife. He rinsed it under water, applied pressure until the bleeding stopped, and covered it with a bandage—thinking little of it. But three days later, the cut had become hot to the touch, the surrounding skin was increasingly red, and the pain had intensified rather than improved.
“I assumed it would get better on its own,” Alex told us. “By the time I saw a doctor, I needed antibiotics and nearly ended up in the hospital.”
Understanding the difference between normal healing and infection isn’t just about comfort—it can prevent serious complications including cellulitis, sepsis, and even limb loss. This evidence-based guide will help you recognize the warning signs that require medical attention.
Dealing with a wound that won't heal?
We'll help connect you with a wound care practice near you — free, no obligation.
Find a Practice Near You2. Quick Reference Guide
| Question | Evidence-Based Answer |
|---|---|
| Is some redness normal? | Yes. Mild redness immediately around the wound edges that gradually diminishes is part of normal inflammatory response. |
| Is clear fluid normal? | Yes. Clear or slightly yellow fluid during the first 48-72 hours is normal wound exudate. |
| When do I need medical attention? | For any: spreading redness beyond 1 inch of the wound; increased pain after 48 hours; thick, opaque, or foul-smelling discharge; red streaks; fever; or deep wounds. |
| What if I have diabetes or immunosuppression? | Seek professional care for ANY suspected infection, as symptoms may be subtle and complications develop more rapidly. |
| What can I do at home? | Monitor daily, clean properly, use appropriate dressings, and know the warning signs that necessitate medical care. |
3. The Science of Infection vs. Healing
Understanding Normal Wound Healing
Wound healing follows four distinct phases, each with normal signs that might be mistaken for infection:
Phase 1: Hemostasis (0-several hours) Blood vessels constrict and platelets form clots to stop bleeding. You’ll see:
- Blood clotting
- Initial wound contraction
Phase 2: Inflammation (1-5 days) Your immune system activates to clean the wound. Normal signs include:
- Redness directly around the wound
- Mild swelling
- Slight warmth
- Mild pain
- Clear or slightly yellow fluid (serous exudate)
- These symptoms should gradually IMPROVE, not worsen, after the first 48 hours
Phase 3: Proliferation (5-21 days) Your body builds new tissue. You’ll observe:
- Reduced redness and swelling
- Pink or red tissue forming in the wound base
- Wound edges contracting
- Decreased fluid
- Reduced pain
Phase 4: Remodeling (21 days to 2 years) The final healing phase includes:
- Scar tissue formation and maturation
- Gradual fading of redness to pink, then white or silvery
- Return of some skin strength
How Infection Disrupts Normal Healing
When pathogens overwhelm your body’s defenses, the inflammatory phase becomes prolonged and exaggerated. Key differences in infected wounds:
- Normal inflammation is localized, peaks at 48-72 hours, then gradually resolves
- Infection causes intensifying symptoms, spreading inflammation, and tissue destruction
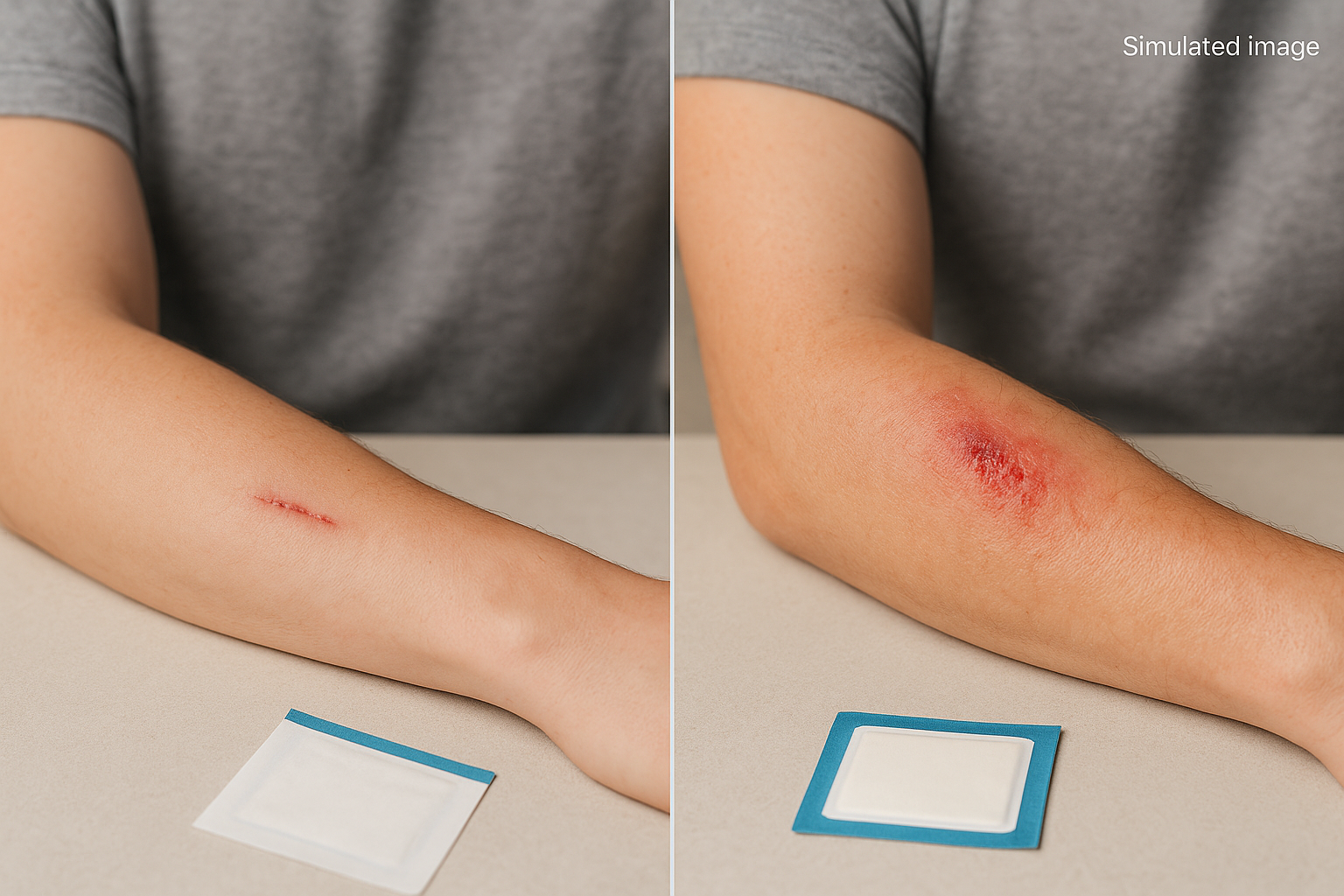
4. Visual Comparison: Normal Healing vs. Infection
Normal Wound Healing Timeline with Visual Markers
| Timeline | Normal Appearance | Normal Sensations | What’s Happening |
|---|---|---|---|
| 0-24 hours | • Red wound edges • Possible slight bleeding or clear fluid • Visible wound edges | • Sharp pain that improves with time • Tenderness when touched | Blood cells form clots and your immune system activates |
| 24-72 hours | • Slightly swollen • Red within 1/4 inch of wound edges • Clear or slightly yellow drainage • Possible scab formation beginning | • Decreasing pain • Mild warmth around wound • Slight throbbing sensation | Inflammatory cells clean debris and fight potential pathogens |
| 3-5 days | • Decreasing redness • Scab formation or moist pink/red tissue if covered • Reduced drainage | • Mild discomfort • Possible slight itching • Less tenderness | New blood vessels forming, collagen production begins |
| 5-10 days | • Minimal redness • Wound noticeably smaller • Pink or red healthy granulation tissue • Minimal drainage | • Occasional itching • Minimal pain • Slight pulling sensation | New skin cells migrate across wound surface, wound contracts |
| 10-21 days | • New skin forming from edges or across surface • Pink coloration • Minimal or no drainage | • Occasional itching • Minimal to no pain | Complete closure for simple wounds, continued healing for larger wounds |
Warning Signs of Infection (Visual Indicators)
| Infection Sign | What It Looks Like | What’s Happening | Urgency Level |
|---|---|---|---|
| Increasing Redness | • Redness expands beyond initial area • Intensifies rather than fades • Spreads more than 1/2 inch beyond wound edges | Inflammatory response to bacterial invasion | Seek medical care within 24 hours |
| Warmth/Heat | • Noticeably warmer than surrounding skin • Heat may radiate several inches from wound | Increased blood flow due to inflammatory cytokines | Seek medical care within 24 hours |
| Purulent Drainage | • Thick, opaque fluid • Yellow, green, or brown color • May have foul odor | Accumulation of white blood cells, bacteria, and dead tissue | Seek medical care within 24 hours |
| Increasing Pain | • Pain intensifies after 48 hours • Pain with gentle pressure • Throbbing, pulsing sensation | Inflammatory mediators and pressure from edema stimulate pain receptors | Seek medical care within 24 hours |
| Swelling | • Pronounced puffiness around wound • Shiny, taut skin • Indentation when pressed | Increased vascular permeability causing fluid accumulation | Seek medical care within 24 hours |
| Red Streaking | • Red lines moving away from wound toward heart • Often following visible veins or lymphatic channels | Lymphangitis – inflammation of lymphatic vessels | EMERGENCY – Seek immediate medical care |
| Fever/Chills | • Body temperature >100.4°F (38°C) • Possible shivering, weakness | Systemic inflammatory response to infection | EMERGENCY – Seek immediate medical care |
5. Evidence-Based Assessment Tool: Is Your Wound Infected?
Use this assessment checklist to evaluate your wound. If you check ANY boxes in the “Warning Signs” column, contact a healthcare provider.
| Observation | Normal Healing Signs | Warning Signs of Infection |
|---|---|---|
| Redness | □ Limited to wound edges □ Fading daily after first 48 hours | □ Expanding beyond initial area □ Intensifying rather than fading<br>□ Spreading more than 1/2 inch from edges |
| Drainage | □ Clear or slightly yellow fluid □ Decreasing in amount □ No odor | □ Thick, opaque yellow/green discharge □ Increasing in amount □ Foul-smelling |
| Pain | □ Gradually decreasing □ Responds to basic pain relievers | □ Intensifying after 48 hours □ Throbbing or pulsing □ Not relieved with pain medication |
| Swelling | □ Mild, limited to wound edges □ Decreasing daily after first 48 hours | □ Pronounced and spreading □ Firm or hard to touch □ Increasing after 48 hours |
| Temperature | □ Slight warmth directly around wound | □ Noticeably hot to touch □ Heat extending beyond wound edges |
| Systemic Signs | □ Normal body temperature □ Normal energy levels | □ Fever >100.4°F (38°C) □ Chills □ Unusual fatigue |
| Wound Appearance | □ Wound edges coming together □ Pink or red tissue in base | □ Wound edges separating or opening wider □ Gray, white, or dark tissue in wound base |
| Lymph Involvement | □ No visible changes along lymph pathways | □ Red streaks extending from wound □ Swollen lymph nodes (groin, armpit, neck) |
Immediate Medical Attention Required For:
- Red streaking extending from wound
- Fever above 100.4°F (38°C)
- Significant swelling, especially if warm to touch
- Inability to move joint near wound
- Increased pain after 48 hours
- Any symptoms in persons with diabetes, immune disorders, or circulation problems
6. Proper Wound Care Protocols to Prevent Infection
Follow these evidence-based wound care steps to minimize infection risk:
Initial Wound Care
- Wash Your Hands Thoroughly – Use soap and water for at least 20 seconds before touching the wound or supplies.
- Stop the Bleeding – Apply gentle, direct pressure with a clean cloth or bandage for 15-20 minutes.
- Clean the Wound Properly:
- Use running potable water or sterile saline solution
- Gently clean with mild soap (avoid harsh soaps or antiseptics)
- Clean from center outward to avoid introducing contaminants
- Rinse thoroughly to remove all soap residue
- Need detailed instructions? See our full wound-cleaning guide.
- Assess the Wound:
- Depth: If deeper than 1/4 inch, seek medical attention
- Debris: Remove visible particles gently with tweezers sterilized in alcohol
- Edges: Note how edges align for monitoring purposes
- Apply Appropriate Dressing:
- Choose based on wound type, location, and drainage. Not sure what bandage to use? Check our full guide to wound coverings.
Ongoing Care
- Monitor Daily – Check for infection signs using the assessment tool above.
- Change Dressings Properly:
- Wash hands before and after
- Remove old dressing by pulling parallel to skin, not away from it
- Clean wound with each dressing change
- Apply new sterile dressing according to type
- Consider Evidence-Based Natural Remedies as adjuncts to proper dressing:
- Medical-grade Manuka honey (UMF 15+) has proven antibacterial properties
- Curious what actually helps? Explore natural wound care that works.
- Optimize Healing Environment:
- Keep wound appropriately moist (not too wet, not too dry)
- Maintain stable temperature
- Protect from excessive movement or pressure
7. High-Risk Wounds: When Standard Rules Don’t Apply
Some wounds and patient conditions require more vigilant monitoring and lower thresholds for seeking medical care:
High-Risk Wound Types
| Wound Type | Why It’s High-Risk | Modified Action Threshold |
|---|---|---|
| Puncture Wounds | • Deep with small surface area • Difficult to clean • Can trap bacteria in deep tissues | Seek medical care for ANY puncture deeper than 1/4 inch, especially on foot |
| Animal/Human Bites | • High bacterial load • Risk of unusual pathogens • Crushing injury component | Seek medical care for ALL bites that break skin, regardless of size |
| Contaminated Wounds | • Foreign material embedded • Contact with soil, feces, etc. • Increased bacterial load | Seek medical care for wounds with debris that cannot be fully removed |
| Surgical Wounds | • Direct access to deep tissues • Possible involvement of organs or implants | Contact surgeon for ANY unexpected changes in appearance, drainage, or sensation |
| Wounds Near Joints | • Movement disrupts healing • Potential for joint space contamination | Seek care for wounds crossing joint lines that show ANY infection signs |
High-Risk Patient Factors
| Patient Factor | Why It’s High-Risk | Modified Action Threshold |
|---|---|---|
| Diabetes | • Impaired immune response • Reduced wound sensation • Poor circulation | Seek care for ANY suspected infection, even with subtle signs |
| Immunosuppression | • Weakened immune defenses • Muted inflammatory response • Atypical presentation | Seek care for ANY signs of infection, regardless of severity |
| Peripheral Vascular Disease | • Reduced blood flow to extremities • Impaired delivery of immune cells • Poor nutrient delivery | Seek care for wounds on extremities that don’t show improvement within 24-48 hours |
| Age >65 Years | • Skin fragility • Reduced immune efficiency • Slower healing response | Lower threshold for seeking care with any concerning symptoms |
| Malnutrition | • Inadequate protein for tissue repair • Micronutrient deficiencies • Reduced collagen formation | Seek care for wounds showing ANY delayed healing signs |
8. Evidence-Based Home Care Products
| Product Type | When to Use | How to Choose | Application Tips |
|---|---|---|---|
| Wound Cleansers | Initial cleaning and with dressing changes | • Sterile saline solution • Mild soap and water • Avoid hydrogen peroxide, alcohol, or povidone-iodine on open wounds | • Irrigate gently • Use room temperature solution • Clean from center outward |
| Antimicrobial Dressings | For wounds at high risk of infection or with early infection signs | • Silver-impregnated dressings • Iodine-based dressings • PHMB-containing dressings | • Follow manufacturer’s directions • Note: Not for long-term use without medical supervision |
| Advanced Wound Coverings | Based on wound type, location, and drainage | • Refer to our Wound Dressing Guide for detailed dressing selection • Match dressing to exudate level | • Cover wound completely with 1-2cm margin • Secure without excessive pressure |
| Medical-Grade Honey | For wounds with minor signs of bacterial contamination | • UMF 15+ or MGO 400+ Manuka honey • Medical-grade only (not food-grade) | • Apply thin layer directly or on dressing • See our Natural Remedies Guide for protocols |
| Skin Protectants | For skin around wound to prevent maceration or irritation | • Zinc oxide creams • Petroleum-based barriers • Silicone-based protectants | • Apply to intact skin only • Create 1-2cm barrier around wound edges |
👉 For a complete guide to evidence-based dressings for different wound types, see our Wound Dressing Guide.
9. When to Seek Professional Care: Decision Tree
SEEK EMERGENCY CARE IMMEDIATELY IF:
- Red streaks moving away from the wound
- Fever above 100.4°F (38°C) with a wound
- Significant swelling with warmth and pain
- Inability to move a joint near the wound
- Any signs of infection in wounds on the face
- Foul odor with dark or black tissue
- Signs of infection in someone with diabetes or immune system disorders
SEEK CARE WITHIN 24 HOURS IF:
- Increasing pain after the first 48 hours
- Spreading redness beyond 1/2 inch of wound edges
- Thick yellow, green, or brown discharge
- Wound that was closing begins to open again
- Increasing warmth around the wound
- Numbness or tingling that wasn’t present earlier
SCHEDULE A ROUTINE APPOINTMENT IF:
- Wound hasn’t shown significant improvement in 7-10 days
- You’re uncertain about proper wound care techniques
- You need assistance choosing appropriate dressings
- You have questions about scar management
What to Expect at Your Appointment:
- Physical examination of the wound
- Possible wound culture if infection is suspected
- Cleaning and debridement if needed
- Prescription medications if indicated
- Instructions for continued home care
10. Nutrition & Lifestyle Factors That Prevent Infection
Evidence-Based Nutritional Support
| Nutrient | Food Sources | How It Prevents Infection |
|---|---|---|
| Protein | Lean meats, fish, eggs, legumes, dairy | Provides building blocks for immune cells and antibodies; clinical studies show inadequate protein increases infection risk by 25-40% |
| Vitamin C | Citrus fruits, bell peppers, strawberries, broccoli | Powers neutrophil function and enhances bacterial killing; deficiency increases infection rates by 30% in clinical studies |
| Zinc | Oysters, beef, pumpkin seeds, lentils | Critical for immune cell development and function; supplementation reduced wound infection rates by 20% in at-risk patients |
| Vitamin A | Sweet potatoes, carrots, spinach, liver | Maintains epithelial barriers and regulates inflammation; deficiency linked to 3x higher infection rates in surgical wounds |
| Vitamin D | Fatty fish, fortified foods, sunshine | Activates antimicrobial peptides; low levels associated with 2x higher surgical site infection rates |
Lifestyle Factors That Significantly Impact Infection Risk
- Blood Glucose Control: Studies show each 1% increase in HbA1c above normal correlates with a 30% higher infection risk.
- Smoking Cessation: Research demonstrates smoking increases wound infection risk by 2-6 times due to tissue hypoxia and impaired neutrophil function.
- Hydration: Clinical evidence indicates dehydration impairs wound healing and increases infection susceptibility by compromising circulation and cellular function.
- Stress Management: Psychological stress increases cortisol, which suppresses immune function; studies show stress management can reduce infection rates by 15-20%.
- Hand Hygiene: Proper handwashing before wound care reduces infection risk by 50% according to multiple clinical studies.
11. Comprehensive FAQ: Expert Answers
Q: How can I tell the difference between normal wound drainage and pus?
A: Normal drainage (exudate) is clear, thin, and watery or slightly yellow. It typically decreases over time. Pus is thick, opaque, and yellow, green, or brown. It may have an unpleasant odor and often increases rather than decreases. If you’re uncertain, take a photo to track changes or consult a healthcare provider.
Q: Are all infected wounds painful?
A: Not necessarily. While increased pain is a common symptom of infection, people with neuropathy (nerve damage) may have reduced sensation. This is particularly concerning in patients with diabetes, who may develop serious infections with minimal pain. In these cases, visual signs become even more important.
Q: Can I use hydrogen peroxide or alcohol to prevent infection?
A: No. Despite popular belief, these products can damage healthy cells and delay healing. Multiple clinical studies show they cause more harm than benefit. Instead, use sterile saline or clean running water with mild soap, which clean wounds effectively without damaging tissue.
Q: How soon after injury does infection develop?
A: Infection typically becomes apparent 2-5 days after injury, but can develop as early as 24 hours or as late as 2 weeks after, depending on the pathogen, wound characteristics, and host factors. This is why daily monitoring is crucial.
Q: Should I remove a scab if it looks infected underneath?
A: Never forcibly remove a scab. If you suspect infection under a scab, seek medical care. Healthcare providers can safely assess and treat the wound without causing additional trauma.
Q: Can small wounds lead to serious infections?
A: Absolutely. Even tiny punctures or cuts can develop serious infections, particularly if they’re deep, contaminated, or on a high-risk body area. Size does not determine infection risk—location, depth, cleanliness, and host factors are more important determinants.
Q: Is it better to keep a wound covered or let it “breathe”?
A: Research conclusively shows that covered wounds heal faster and have lower infection rates than uncovered wounds. The “let it breathe” approach is an outdated myth. Modern wound care focuses on maintaining a moist (not wet) healing environment, which requires appropriate dressings. See our Wound Dressing Guide for specific recommendations.
Q: Can I use essential oils to prevent wound infection?
A: While some essential oils show antimicrobial properties in laboratory studies, clinical evidence does not support their direct application to open wounds. Many essential oils are cytotoxic to human cells and can cause irritation or allergic reactions. For evidence-based natural approaches, see our Natural Remedies Guide.
12. Expert Perspectives on Wound Infection
Dr. Maria Rodriguez, MD, FACS, Surgical Wound Specialist
“What many patients don’t realize is that the window for intervention is critical. If you catch infection in the first 24-48 hours, oral antibiotics and proper wound care can usually resolve it quickly. Wait too long, and you might need IV antibiotics, surgical debridement, or hospitalization. I advise my patients to take daily photos of concerning wounds to track subtle changes that might otherwise go unnoticed. This visual documentation is incredibly helpful for both patients and clinicians.”
Professor James Thompson, PhD, Clinical Microbiology
“The microbiome of a wound changes dramatically as infection develops. Initially, a diverse population of microorganisms might be present without causing harm. But when conditions favor certain pathogens—particularly Staphylococcus aureus, Streptococcus species, or Pseudomonas aeruginosa—they can quickly overwhelm the body’s defenses. What’s concerning is the rise in antibiotic-resistant strains, making prevention more crucial than ever. This is why proper cleaning, appropriate dressing selection, and early intervention remain the gold standards for preventing serious infections.”
Sarah Johnson, RN, WCC, Wound Care Nurse
“In my practice, I find that patients often miss the early signs of infection because they’re looking for the wrong things. They wait for dramatic pus or severe pain, when subtle changes like slightly increased warmth or a change in wound odor might be the first indicators. I teach my patients to use all their senses when assessing wounds—visual changes, temperature differences, new smells, and evolving sensations. This comprehensive approach helps catch infections before they become serious.”
13. Resources & Top Articles:
- How to Clean Any Wound at Home
- Guide to Wound Dressings
- How to Tell If a Wound Is Infected
- Natural Remedies for Wound Healing
14. Comprehensive Summary
- Know the difference: Normal healing involves limited redness, clear drainage, and improving symptoms. Infection causes spreading redness, increasing pain, and often thick, discolored discharge.
- Monitor systematically: Check your wound daily, comparing to previous days to detect subtle changes. Use the assessment tool provided in Section 5.
- Use evidence-based care: Proper cleaning, appropriate dressing selection, and maintenance of a moist healing environment significantly reduce infection risk. See our Wound Dressing Guide for specific recommendations.
- Consider selective natural approaches: Some natural remedies like medical-grade honey have strong clinical evidence for infection prevention. See our Natural Remedies Guide for science-backed options.
- Recognize high-risk scenarios: Certain wound types and patient factors require higher vigilance and lower thresholds for seeking care.
- Act promptly: Early intervention dramatically improves outcomes and reduces complications. Don’t delay seeking care if warning signs appear.
15. References and Further Reading
- Centers for Disease Control and Prevention (CDC). (2023). Wound Infection Prevention Guidelines.
- World Union of Wound Healing Societies. (2024). Consensus Document: Identification and Management of Wound Infection.
- Lindholm, C., & Searle, R. (2023). “Wound infection and diagnostics.” International Wound Journal, 18(2), 17-31.
- Murphy, C., et al. (2024). “Clinical assessment tools for identification of local wound infection: A critical review.” Wounds International, 12(3), 43-58.
- Robson, V., Dodd, S., & Thomas, S. (2009). “Standardized antibacterial honey (Medihoney) with standard therapy in wound care: Randomized clinical trial.” Journal of Advanced Nursing.
- Kordestani, S.S., et al. (2008). “A randomised controlled trial on the effectiveness of an advanced wound dressing used in Iran.” Journal of Wound Care.
- European Wound Management Association. (2024). Position Document: Identifying Criteria for Wound Infection.
- Wounds UK. (2024). Best Practice Statement: Antimicrobial Stewardship Strategies for Wound Management.
- Gardner, S.E., et al. (2022). “Clinical signs of infection in diabetic foot ulcers: An analysis of reliability and validity.” Advances in Skin & Wound Care.
- International Working Group on the Diabetic Foot. (2023). Guidelines on Prevention and Management of Diabetic Foot Infections.
Related answers
- A Transparent Film Dressing Is Used for Which Type of Wound?
- Does Alcohol Affect Wound Healing?
- Evidence-Based Natural Remedies for Wound Healing
- How to Clean Any Wound at Home: Evidence-Based Guide
This content is for educational purposes only and is not a substitute for professional medical advice. Always consult a qualified healthcare provider about your wound.