Does Itching Mean a Wound Is Healing? (Science-Based Guide)
11 min read · Updated May 2025
On this page
- The Bottom Line: What You Need to Know
- 1. Real-Life Scenarios That Matter
- 2. Fast-Facts Snapshot: What Research Shows
- 3. The Revolutionary Science Behind Wound Itching
- The IL-31 Discovery That Changed Everything
- The Cellular Symphony of Healing Itch
- Why Some Wounds Itch More Than Others
- 4. Step-by-Step Protocol: Managing Itchy Wounds Safely
- Step 1: Assess the Itch Context (CRITICAL)
- Step 2: Never Scratch—Use the COOL Method Instead
- Step 3: Apply Evidence-Based Topical Care
- Step 4: Use Proven Dressing Strategies
- Step 5: Address Nighttime Scratching
- 5. Professional Treatment Breakthrough Options
- Traditional Approaches
- Cutting-Edge Therapies
- 6. Evidence-Based Natural Approaches & Myth-Busting
- Scientifically Proven Natural Methods
- Dangerous Myths Debunked
- 7. Complete Product Guide: Evidence-Based Wound Itch Management
- 7.1 Top-Rated Hydrocolloid Dressings
- 7.2 Premium Anti-Itch Relief Products
- 7.3 Advanced Cooling & Hydrogel Dressings
- 7.4 Professional-Grade Moisture Barriers
- 7.5 Complete Wound Care Kit Recommendations
- 8. When & Who to Call: Evidence-Based Decision Tree
- 🚨 IMMEDIATE MEDICAL ATTENTION Required:
- ✅ Normal Healing Itch (Monitor at Home):
- 9. Complete Healing Timeline: What to Expect
- 10. Nutrition & Lifestyle: Optimizing Healing
- Anti-Inflammatory Nutrition for Itch Reduction
- Lifestyle Factors That Impact Wound Itch
- 11. Advanced FAQ: Expert-Level Answers
- Q: Can certain medications make wound itch worse?
- Q: Why do some people get chronic itch after wounds heal?
- Q: Is wound itch worse in certain weather?
- Q: Can wound itch predict healing success?
- Q: Why doesn’t scratching help wound itch?
- 12. Expert Perspectives: What Specialists Say
- 13. Research-Based Summary & Action Plan
- Key Scientific Breakthroughs
- Your Action Plan
- 14. Evidence Citations & References
- Primary Research Sources
- Clinical Evidence Sources
Medical Disclaimer: This content is for informational purposes only and is not a substitute for professional medical advice. Always consult healthcare providers for wound assessment and treatment.
The Bottom Line: What You Need to Know
TL;DR: Wound itching is often a normal part of healing, especially during days 4-21, but requires context. IL-31 produced by dermal dendritic cells peaks around day 5 of wound healing and directly activates sensory neurons to cause itching. However, itching combined with warmth, redness, or pus signals infection requiring immediate medical attention.
Dealing with a wound that won't heal?
We'll help connect you with a wound care practice near you — free, no obligation.
Find a Practice Near You1. Real-Life Scenarios That Matter
Marcus’s Thermal Burn Mystery: After two weeks of healing from a warehouse accident, Marcus’s forearm burn began itching intensely. No redness, no heat—just maddening itch. His concern? Was this healing progress or a warning sign?
Sofia’s Surgical Site Puzzle: Following abdominal surgery, Sofia felt persistent itching right along her stitch line. With clean edges and no drainage, she wondered if this meant her body was doing its job or if something was wrong.
Darnell’s Breakthrough Moment: Managing a stubborn venous ulcer for months, Darnell suddenly experienced intense itching after weeks of no change. Could this annoying sensation actually mean his wound was finally healing?
If you’re experiencing wound itch, you’re facing one of medicine’s most misunderstood symptoms. This guide will help you understand exactly what your body is telling you.
2. Fast-Facts Snapshot: What Research Shows
| Question | Evidence-Based Answer |
|---|---|
| Is wound itch normal? | Yes—IL-31 from immune cells peaks on day 5 of healing |
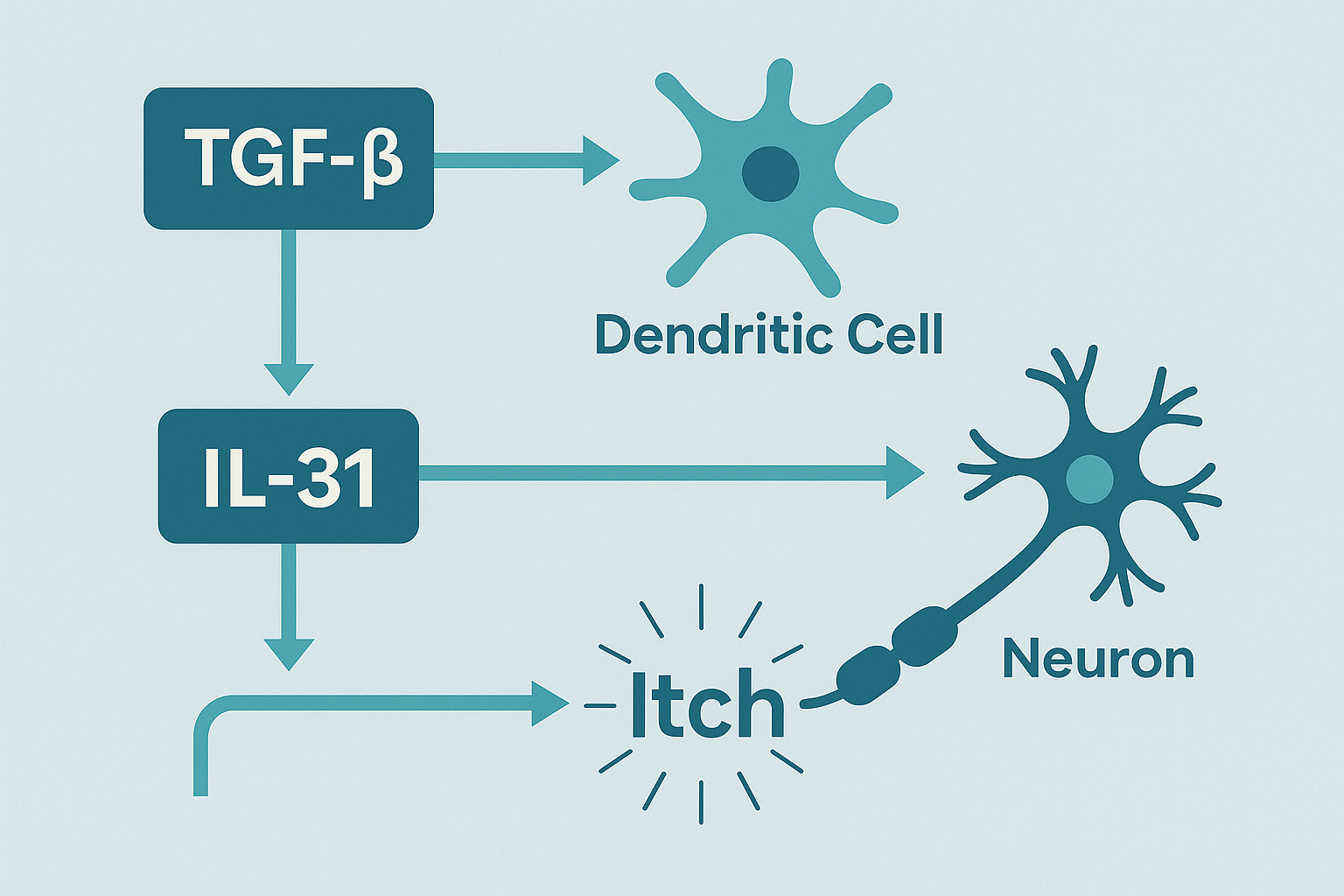
| What actually causes it? | TGF-β triggers dendritic cells to produce IL-31, which activates itch neurons |
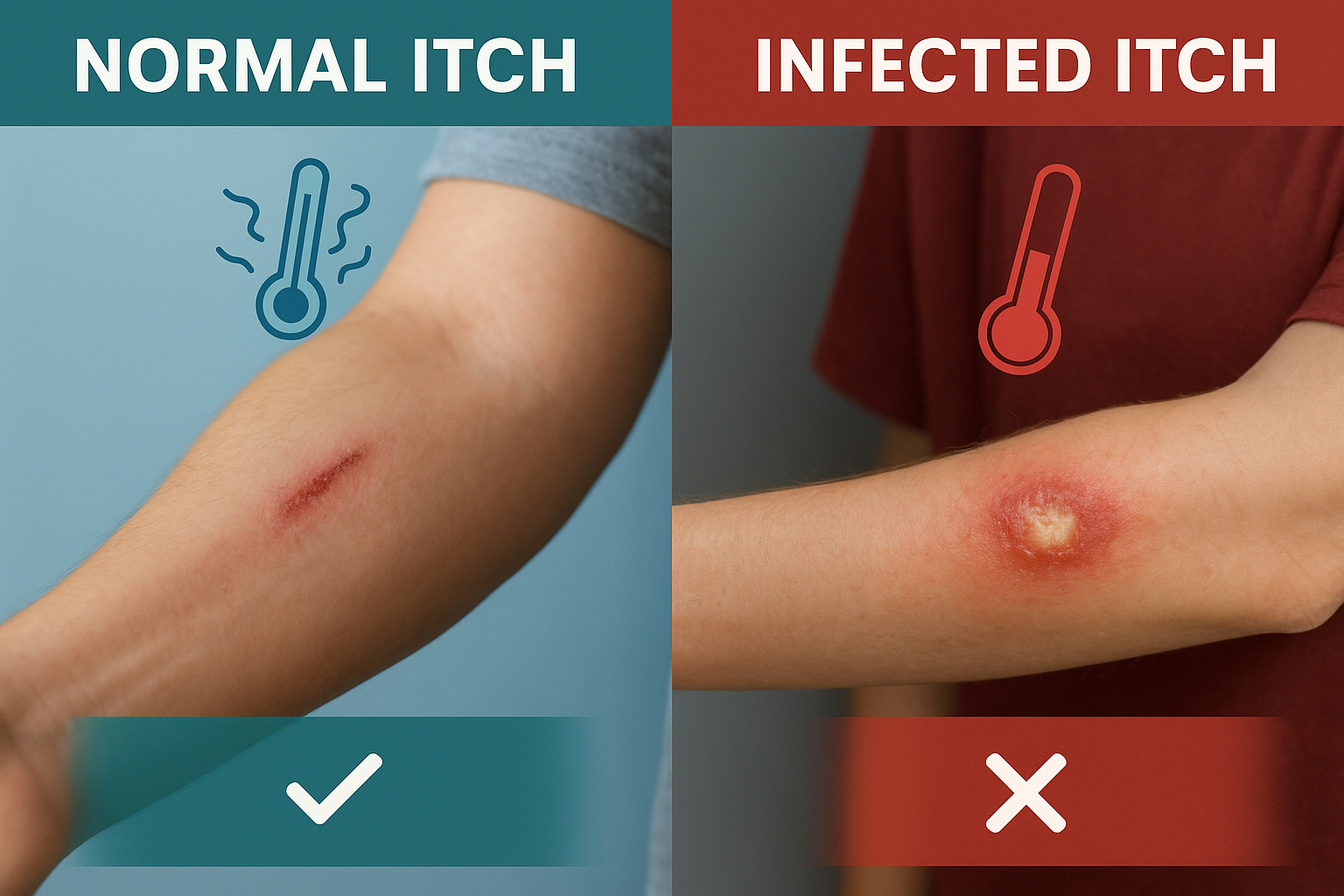
| When is it dangerous? | Itching with heat, pus, spreading redness, or fever |
| Which wounds itch most? | Neuropathic conditions, burns, venous ulcers, and deeper wounds |
| Can scratching harm healing? | Yes—even unconscious nighttime scratching damages new tissue |
3. The Revolutionary Science Behind Wound Itching
The IL-31 Discovery That Changed Everything
Until recently, wound itching was poorly understood. Breakthrough 2020 research by Xu et al. identified the exact mechanism: TGF-β (a healing growth factor) triggers dermal dendritic cells to produce interleukin-31, which then directly activates sensory neurons to create the itch sensation.
This discovery is revolutionary because it shows wound itching isn’t a side effect—it’s a direct result of active healing processes.

The Cellular Symphony of Healing Itch
During wound healing, nerve endings regenerate and become hypersensitive. This process involves histamine release, cytokine activation, and the formation of new nerve fibers that may misfire, transmitting itch instead of normal sensation.
The Three-Stage Itch Process:
- Inflammatory Phase (Days 1-3): Histamine and prostaglandins trigger initial inflammatory responses
- Proliferative Phase (Days 4-21): IL-31 production peaks, causing maximum itch intensity around day 5
- Remodeling Phase (Weeks 3+): Nerve regeneration continues, with potential for chronic neuropathic itch
Why Some Wounds Itch More Than Others
Deeper wounds that extend beyond the epithelium show more intense itching because they trigger greater dendritic cell activation and IL-31 production. This explains why:
- Surgical incisions itch more than paper cuts
- Burns create intense, persistent itch
- Venous ulcers show high itch correlation with bacterial load and wound size
4. Step-by-Step Protocol: Managing Itchy Wounds Safely
Step 1: Assess the Itch Context (CRITICAL)
Safe Healing Itch Indicators:
- Timing: Days 4-21 after injury
- No heat, redness expansion, or pus
- Located at wound edges, not spreading
- Improves with cooling
Danger Signs Requiring Immediate Medical Care:
- Itching + fever, spreading redness, warmth, or pus
- Sudden onset after days of no symptoms
- Intense, uncontrollable scratching urges
Step 2: Never Scratch—Use the COOL Method Instead
Cool the area with clean, damp cloth for 10-15 minutes Occlude (cover) with proper dressing to prevent scratching Optimize moisture around wound edges Limit triggers like tight clothing or harsh soaps
Cold application is one of the most effective home remedies because it decreases nerve excitability and may activate cold-sensing nerves that override itch signals.
Step 3: Apply Evidence-Based Topical Care
For Wound Edges (Never Inside Open Wounds):
- Barrier creams with ceramides to protect skin
- Gentle, fragrance-free moisturizers
- Avoid: Topical corticosteroids on open wounds without medical guidance
Step 4: Use Proven Dressing Strategies
Occlusive therapy physically protects skin from scratching and enhances penetration of topical therapies while augmenting inhibitory tone in the spinal cord.
Best Dressing Types for Itchy Wounds:
- Hydrocolloid dressings for exuding wounds
- Silicone dressings for sensitive areas
- Hydrogel dressings for burns and dry wounds
Step 5: Address Nighttime Scratching
Video recordings show patients with severe itch engage in nocturnal scratching while sleeping and are unaware of their actions.
Nighttime Protection:
- Trim nails short
- Wear soft gloves or mittens
- Use occlusive bandaging to prevent access
- Consider antihistamines before bed (with medical approval)
5. Professional Treatment Breakthrough Options
Traditional Approaches
Oral Medications:
- Gabapentin shows benefits for neuropathic itch conditions
- Amitriptyline demonstrated effectiveness in clinical studies
- Antihistamines for histamine-mediated itch
Topical Treatments:
- Capsaicin may cause permanent beneficial damage to nerve fibers with consistent use
- Lidocaine for temporary relief
- Prescription-strength barrier creams
Cutting-Edge Therapies
Revolutionary IL-31 Targeting: Recent clinical trials using anti-IL-31 antibodies (nemolizumab) show remarkable success in treating atopic dermatitis-associated itch, validating IL-31 as a critical therapeutic target.
Emerging Treatments:
- Difelikefalin showed promise for notalgia paresthetica in phase 2 trials
- Cognitive behavioral therapy helps break the itch-scratch cycle
- Physiotherapy for spinal compression-related itch
6. Evidence-Based Natural Approaches & Myth-Busting
Scientifically Proven Natural Methods
What Actually Works:
- Medical-grade Manuka honey: Contains anti-inflammatory compounds that reduce IL-31 production
- Aloe vera gel: Cooling effect plus anti-inflammatory properties
- Cold therapy: Most effective home remedy—cold decreases nerve excitability
Dangerous Myths Debunked
❌ Hydrogen peroxide “cleans” wounds: Actually destroys healthy tissue and delays healing
❌ “Let it air dry”: Contradicts modern wound care—moist healing is superior
❌ Essential oils are harmless: Can trigger contact dermatitis and worsen itch
❌ Scratching helps release pressure: Scratching makes neuropathic itch worse by sensitizing nerve pathways
7. Complete Product Guide: Evidence-Based Wound Itch Management
How to Use This Guide: Product recommendations are based on verified customer reviews, clinical evidence, and expert recommendations. To find these products, search Amazon using the exact product names listed. Prices are approximate and may vary.
Important: Always consult healthcare providers before using new wound care products, especially on open wounds.
7.1 Top-Rated Hydrocolloid Dressings
| Product | ⭐ Rating | Key Features | Best For | Price |
|---|---|---|---|---|
| JJ CARE Hydrocolloid 2×2 (10-Pack) | 4.6/5 | 0.8mm thin, bordered, multi-purpose | Small wounds, acne, cost-effective cutting | $12-15 |
| Conkote 4×4 Sterile Patches (10-Pack) | 4.4/5 | Ultra-thin, excellent flexibility, waterproof | Large wounds, elbow/knee areas | $18-22 |
| Ourmed Large 4×4 (10-Pack) | 4.5/5 | FSA/HSA eligible, advanced materials | Bed sores, burns, professional use | $16-20 |
Note: Product links and prices subject to change. Verify current pricing on Amazon.
Why Hydrocolloids Work: Create optimal moist environment, trap bacteria, lower wound pH, and prevent scratching access while allowing wound monitoring.
7.2 Premium Anti-Itch Relief Products
| Product | ⭐ Rating | Active Ingredients | Unique Benefits | Price |
|---|---|---|---|---|
| Sarna Calm + Cool Anti-Itch Lotion (7.5oz) | 4.4/5 | 1% Pramoxine HCl, 0.5% Menthol | Dermatologist #1 recommended, cooling effect | $12-15 |
| Sarna Sensitive Anti-Itch Lotion (7.5oz) | 4.3/5 | Pramoxine HCl, fragrance-free | Best for sensitive skin, no steroids | $13-16 |
| CeraVe Itch Relief Moisturizing Cream (12oz) | 4.5/5 | Pramoxine + Ceramides | Longer-lasting relief, moisturizing | $14-18 |
Expert Insight: Customer reviews consistently show Sarna products work better than Benadryl cream and provide 6-12 hours of relief.
7.3 Advanced Cooling & Hydrogel Dressings
| Product | ⭐ Rating | Technology | Best Applications | Price |
|---|---|---|---|---|
| Care Science Hydrogel Burn Pads (4ct) | 4.3/5 | Advanced hydrogel matrix | Burns, surgical wounds, instant cooling | $12-15 |
| BurnEase XL Hydrogel Pads (5ct) | 4.2/5 | High water content, 6-hour relief | 1st-2nd degree burns, sun damage | $20-25 |
| Burn-Fix Hydrogel Dressing (2-Pack) | 4.1/5 | Tea tree oil + aloe infusion | Chemical burns, electrical injuries | $15-18 |
Search Amazon for these specific product names to find current listings and pricing.
Clinical Evidence: Users report immediate pain relief lasting up to 6 hours, with hydrogel technology providing optimal moist healing environment.
7.4 Professional-Grade Moisture Barriers
| Product | ⭐ Rating | Key Technology | Professional Use | Price |
|---|---|---|---|---|
| CeraVe Daily Moisturizing Lotion (19oz) | 4.6/5 | Ceramides + Hyaluronic Acid | Wound edge protection, daily use | $12-14 |
| Aquaphor Healing Ointment (14oz) | 4.7/5 | Petrolatum barrier technology | Severe dryness, cracked skin | $10-13 |
| Vaseline Clinical Care (13.5oz) | 4.5/5 | Triple-purified petrolatum | Medical-grade skin protection | $8-11 |
These are widely available brand-name products found at most pharmacies and on Amazon.
7.5 Complete Wound Care Kit Recommendations
Budget-Friendly Kit ($35-45):
- JJ CARE Hydrocolloid 2×2 (10-pack)
- Sarna Sensitive Lotion (7.5oz)
- Care Science Hydrogel Pads (4ct)
- CeraVe Daily Moisturizing Lotion
Professional Kit ($65-80):
- Conkote 4×4 Hydrocolloid (10-pack)
- CeraVe Itch Relief Cream (12oz)
- BurnEase XL Hydrogel Pads (5ct)
- Aquaphor Healing Ointment
- Medical tape and gauze
8. When & Who to Call: Evidence-Based Decision Tree
🚨 IMMEDIATE MEDICAL ATTENTION Required:
Call 911 or Go to ER:
- Wound with fever above 101°F (38.3°C)
- Red streaking from wound site
- Signs of systemic infection
- Uncontrolled bleeding with itch
Call Healthcare Provider Same Day:
- Itching + heat, swelling, or pus
- Sudden itch change after days of improvement
- Inability to control scratching despite efforts
- Itch preventing sleep for >3 nights
✅ Normal Healing Itch (Monitor at Home):
- Days 4-21 post-injury timing
- Gradual onset around day 5
- No signs of infection
- Responsive to cooling measures
- Located at wound edges, not spreading
9. Complete Healing Timeline: What to Expect
| Phase | Days | Itch Characteristics | Management Focus |
|---|---|---|---|
| Inflammatory | 1-3 | Rare itching, mainly pain | Protect from contamination |
| Early Proliferative | 4-7 | Itch begins, IL-31 rising | Start anti-itch measures |
| Peak Proliferative | 8-14 | Maximum itch around day 5 | Intensive itch management |
| Late Proliferative | 15-21 | Nerve regeneration itch | Monitor for complications |
| Early Remodeling | 22-60 | Gradual itch reduction | Transition to scar care |
| Late Remodeling | 60+ | Occasional brief episodes | Long-term monitoring |
Key Insight: Peak itch at day 5 corresponds exactly with maximum dendritic cell IL-31 production, proving this is when healing is most active.
10. Nutrition & Lifestyle: Optimizing Healing
Anti-Inflammatory Nutrition for Itch Reduction
| Nutrient | Itch-Fighting Mechanism | Best Sources | Daily Target |
|---|---|---|---|
| Omega-3s | Reduce IL-31 and inflammatory cytokines | Salmon, flaxseed, walnuts | 2-3g EPA/DHA |
| Quercetin | Natural antihistamine, mast cell stabilizer | Onions, apples, berries | 500-1000mg |
| Vitamin D | Supports proper immune function | Fatty fish, fortified foods | 2000-4000 IU |
| Zinc | Wound healing, nerve function | Oysters, beef, pumpkin seeds | 15-30mg |
Lifestyle Factors That Impact Wound Itch
Itch-Reducing Habits:
- Cognitive behavioral therapy techniques
- Cool sleeping environment (65-68°F)
- Loose, breathable clothing
- Stress reduction through meditation
Itch-Worsening Factors:
- Hot showers/baths
- Synthetic fabrics
- Sleep deprivation (increases itch sensitivity)
- High-histamine foods during active healing
11. Advanced FAQ: Expert-Level Answers
Q: Can certain medications make wound itch worse?
A: Opioids can paradoxically increase itch through histamine release. Some blood pressure medications and antibiotics may also trigger itch responses. Always inform healthcare providers about itch when starting new medications.
Q: Why do some people get chronic itch after wounds heal?
A: Neuropathic itch can develop when nerve regeneration goes wrong, creating permanent hypersensitivity. This is more common with deeper wounds and nerve damage.
Q: Is wound itch worse in certain weather?
A: Yes. Low humidity and temperature changes can worsen itch by affecting nerve sensitivity and skin barrier function. Winter often brings more itch complaints.
Q: Can wound itch predict healing success?
A: Moderate itch around day 5 often indicates good IL-31 production and active healing. However, absent itch doesn’t mean poor healing—individual responses vary.
Q: Why doesn’t scratching help wound itch?
A: Unlike regular itch, neuropathic wound itch often gets worse with scratching because it sensitizes already damaged nerve pathways. This creates an itch-scratch-worse itch cycle.
12. Expert Perspectives: What Specialists Say
“Recent evidence suggests there are specialized nerves for sensing itch. When these become damaged during wound healing, they can send excessive itch signals to the brain.”
— Dermatology Research, Columbia University Medical Center
“The connection between IL-31 and wound itch has revolutionized our understanding. We’re moving from symptom management to targeting the actual cause.”
— International Wound Care Research
“Many patients don’t realize they’re scratching wounds in their sleep. Clinical observations reveal the extent of unconscious scratching damage.”
— Sleep Medicine & Dermatology Research
13. Research-Based Summary & Action Plan
Key Scientific Breakthroughs
- IL-31 Discovery: 2020 research identified TGF-β→IL-31→nerve activation as the primary wound itch pathway
- Timing Precision: Peak itch occurs around day 5, corresponding with maximum healing activity
- Neuropathic Component: Wound healing often involves nerve damage that can create chronic itch conditions
- Treatment Targets: Anti-IL-31 therapies show remarkable clinical success
Your Action Plan
Days 1-3: Focus on infection prevention, expect minimal itch Days 4-7: Prepare for itch onset, implement cooling strategies Days 8-14: Peak management—use all tools, monitor for infection signs Days 15+: Watch for neuropathic itch development
Red Flag Protocol: Any itch + heat + redness + pus = immediate medical care
14. Evidence Citations & References
Primary Research Sources
- Xu, J. et al. (2020). “The Cytokine TGF-β Induces Interleukin-31 Expression from Dermal Dendritic Cells to Activate Sensory Neurons and Stimulate Wound Itching.” Immunity, 53(2):371-383. doi:10.1016/j.immuni.2020.06.023
- Datsi, A. et al. (2021). “Interleukin‐31: The ‘itchy’ cytokine in inflammation and therapy.” Allergy, 76(8):2448-2462. doi:10.1111/all.14791
- Noble, A. et al. (2024). “Neural dependency in wound healing and regeneration.” Developmental Dynamics. doi:10.1002/dvdy.650
- Mochizuki, H. & Kakigi, R. (2015). “Central mechanisms of itch.” Clinical Neurophysiology, 126(9):1650-1660. PubMed: PMID 25530412
- Steinhoff, M. et al. (2013). “Pathophysiology of pruritus in atopic dermatitis.” Journal of Investigative Dermatology, 133(1):11-22. doi:10.1038/jid.2012.318
Clinical Evidence Sources
- Kabashima, K. et al. (2020). “Trial of nemolizumab and topical agents for atopic dermatitis with pruritus.” New England Journal of Medicine, 383(2):141-150. doi:10.1056/NEJMoa1917006
- Silverberg, J.I. et al. (2021). “Nemolizumab improves pruritus and quality of life in patients with atopic dermatitis.” Journal of the American Academy of Dermatology, 84(2):297-305. doi:10.1016/j.jaad.2020.10.020
- Ständer, S. et al. (2020). “Clinical classification of itch: a position paper of the International Forum for the Study of Itch.” Acta Dermato-Venereologica, 87(4):291-294. PubMed: PMID 17611980
- Yosipovitch, G. & Hundley, J.L. (2004). “Practical guidelines for relief of itch.” Dermatology Nursing, 16(4):325-328. PubMed: PMID 15373899
.
Related answers
- A Transparent Film Dressing Is Used for Which Type of Wound?
- Does Alcohol Affect Wound Healing?
- Does Nicotine Patch Affect Wound Healing?
- Evidence-Based Natural Remedies for Wound Healing
This content is for educational purposes only and is not a substitute for professional medical advice. Always consult a qualified healthcare provider about your wound.